FIRST AID
FIRST AID
PAGE1
SECTION ONE
STANDARD
FIRST AID
THEORY AND SKILLS
CHAPTER I
THE WHY AND HOW OF FIRST AID
Definition of First Aid
First aid is defined as the immediate and temporary
care given the victim of an accident or sudden illness until
the services of a physician can be obtained.
First aid commences with the steadying effect upon
the stricken person when he realizes that competent hands
will help him. The victim suddenly has new problems and
needs. Often he cannot think well temporarily. Events may
seem unreal and remote. His mind may be dull. The emo-
tonal reaction associated with a serious accident subsides
only gradually. Therefore first aid is more than a dressing
or a splint. It relates to the victim's mind and spirit as well
as to his physical injuries. Its contributions include the well-
selected word of encouragement, the expression of willingness
to help, and the up lift in effect, of the first aider,
voice the immediate problems, the information given con
evident capability. The thoughtful suggestions made to
selfing nearby physicians and hospitals, the telephone ch
co summon medical help of an ambulance or to notify a
relative- these too are first aid.
The good first aider deals with the whole situation, the
person, and the injury. He knows what not to do as well as
what to do. Thus he avoids the etrots so commonly made
through well-meant but misguided efforts. He confines his
procedures to what is necessary, recalling that the handling
injured parts should be kept to a minimum.
The Value of First Aid Training
Value to self
Although many people study first aid in order to help
Others, the training primarily helps the student himself. It
enables him to give proper immediate care to his own
injuries. If he is too seriously injured to help himself, he may
be able to direct others toward proper care. He need not
entrust his injured body to the first aid knowledge of
random passers-by.
First aid training also helps the student by developing
his safety consciousness. Most people recognize the gravity
of our accident problem. Their efforts toward safety, how-
ever, may be occasional and hit-or-miss rather than a part
of a carefully organized plan developed by them for safe
living. The first aid course sharpens the desire for safety,
shows how accidents occur, and focuses attention upon
many specific ways to avoid accidents. A good way to guide
In one toward safety is to have him take a first aid course,
Value to others
Having studied first aid, one is more likely to assist
family members wisely if they are stricken, to give them
some instruction in first aid, and to promote among them a
reasonable safety attitude. While the principal benefits are
to the student and his family, they extend farther, usually,
to co-workers, acquaintances, and strangers. There is always
an obligation on a humanitarian basis to assist the stricken, the helpless.
Value in civil defense
First aid training is recognized as an important aspect
of civil defense. In case of catastrophe, with medical and
hospital service curtailed, citizens must rely largely upon
themselves for a time, caring for their own injuries and for
those of others. Possession of first aid knowledge is a civic
responsibility.
Value in fostering safety consciousness
Disabling accidents, severe enough to cause loss of time
from the usual duties for at least one day after the day of
injury, occur annually in from one-fifth to one-fourth of
our family units. After the first year of life, all through
childhood and early adulthood, accidents are the common-
est cause of death; thereafter they are one of the leading
causes. The rate is about twice as high among males as
females, with many wage-earners affected. The annual
costs for medical and hospital service and direct property
THE WHY AND HOW OF FIRST AID
damage alone total slightly less than one percent of national
personal income. When all wage losses and insurance costs
are added, the total is about three percent. Such costs, year
After a year, greatly affects welfare expenses, and rehabilitation needs.
They reflect the fact that many daily serious
accidents represent an enormous expense and a large number of personal tragedies.
How can first aid help us avoid accidents? Some rea-
sons have already been given. When we spend some hours
studying fractures, head injuries, and burns, we appreciate
with more force what it means to suffer injury. Thereafter
safety programs seem more important and we personalize
their message is better. Thus first aid training fosters force-
fully the safety consciousness that we all need.
General Directions for First Aid
Most accidents are minor and the first aid needed is
obvious to a trained person. In case of serious injury, the
following sequence of action is usually applicable: give the
urgently necessary first aid, have the victim lie down, check
for injuries, plan what to do, and carry out the indicated procedures.
Give urgently necessary first aid
Act quickly for injuries where each second of delay is
important: (a) severe bleeding, (b) stoppage of breathing
where artificial respiration helps, and (c) poisoning. The
proper first aid will be described later. While the first aider's
time and attention are devoted to the patient, someone else
should go or call for a physician: burns, for example-
Other injuries require prompt help. -severe
-but the immediate danger to life is
hot 50 great. The urgent cases are seldom encountered; they
Can usually be recognized and, the first aid requirements
are relatively simple. With most serious accidents, the first
Aider commences with the next step.
Keep the victim lying down
Protect him from unnecessary manipulation and dis-
turbance. Do not heat the patient but keep the body tem-
perature from falling. Blankets beneath are usually more
important than above, but there is hazard in placing them
before you know where the injuries are.
Check for injuries
Your clues are the story of what happened, the vic-
tim's reactions after the accident, his own ideas about his
injuries, and your findings upon examination. The direction
and extent of examination should be guided by the
kind of accident and the needs of the situation. Have a
reason for what you do. If the urgent first aid has been
given and the patient is properly protected pending early
arrival of a physician, a detailed examination is unnecessary.
If you must move the victim even a short distance
before the physician comes, you should first learn what
body parts are injured so that you can support them ade-
quately during the transfer.
Suppose, however, you must carry through with first
aid and perhaps transport the victim. Here you must check
carefully for injuries. Sometimes the task is simple because
it clearly involves a single exposed part, or because, by the
of the accident, there is no possibility of fractures,
pacerations, and the like. An example is poisoning. In other
cases you recognize that any body part may be injured and
require attention. These cases are the accidents caused by
force: for example, traffic accidents, falls, gunshot wounds, blows.
With them, you should assure yourself, through
consideration of the above-mentioned clues, about every
body part--the head, neck, trunk, each extremity in turn.
Remember always to consider head injury and back injury.
With each part, think of surface injury, of fractures, and
of internal organ injury. In addition, note the patient's
general condition and state of consciousness.
Surface injuries are readily evident. Fractures and internal
Organ injuries present greater difficulties. Visual evi-
dence may be lacking with the former and almost always
is with the latter. Therefore your objective in checkup for
them is simple: find what body parts are, or possibly may
be injured. Your first aid should aim to keep these parts
immobile.
Checkup for injuries is far more accurate when the
body part is exposed. Such exposure may be possible in the
home. Utmost caution should be used when clothing is re-
moved, lest added injury result. In public places, with
strangers as victims, exposure of body parts that possibly
may be injured is not generally advisable. In such case you
must act in the light of such knowledge as you can obtain
from the story of the accident, the victim's ideas and re-
actions, and whatever checkup you can make. When in
doubt about a body part, keep it from twisting, bending, and shaking and do not jackknife the patient
Do not pick him up by head and heels.
Plan what to do
"Get a physician or ambulance or obtain medical advice
by telephone. This should be one of the first moves. Discuss
the problem with responsible relatives or friends of the vic:
him who are at hand or briefly with the victim. If helpers
are needed, instruct them carefully in their duties.
Carry out the indicated first aid
Knowing what to do presents few difficulties, once the
the nature and location of the injuries are learned. Do not
attempt to save time and effort by using second-best
methods of first aid for this person entrusted temporarily
to you in his distress. First, stop profuse bleeding and deter-
mine whether artificial respiration is necessary. After that,
one may take time for a more general examination.
Selected additional pointers
Find all the injuries. The checkup is often incomplete
or sketchy after the first injury is found--especially if it
is a major injury.
Give first aid to minor as well as major injuries. For
example, a common error upon finding a fracture of a large
bone and one of a small bone is to splint only the large bone.
Do not give fluids to an unconscious or partly con-
scious person, because they may enter the windpipe. Do not
attempt to rouse an unconscious person by shaking him,
talking, or shouting.
Following injury, do not lift a gasping person by the
belt. This is done very often and may aggravate injuries of
the back or internal organs. Gasping is not always caused by
Image insufficient oxygen but may be due to injury of back or
chest.
'with indoor accidents, use judgment about opening
windows when weather is cold except when noxious gases
are present and may have caused the accident. Indoors or
out, the victim has enough air, and cold air may be too
chilling.
Be reluctant to make statements to the victim and by.
standers about the injuries. It is not the first aider's province
Diagnose, evaluate and predict. Upon questioning from
the victim, you can answer that you would rather have the
physician give information. Helpers must be given neces-.
sary information, however.
Obtain the victim's name and address. When calling
for a physician or ambulance, be sure to give the exact loca-
tion of the injured person, and such information as you
have concerning the nature of the injuries. Be sure that the
physician or ambulance driver knows where to go. Take
advantage of the telephone call to obtain good advice con-
cerning first aid. To avoid missing questions or advice, wait
until the physician or driver hangs up.
Reassure the victim by telling him what first aid steps
you are going to take and how they will help him.
If the victim is unconscious, loosen clothing about his
neck. If there is no fracture turn the patient on his side,
maintaining this position by flexing the leg or legs, and place
a pillow under the head so that secretions may drool from
the corner of the mouth. This will usually allow good res-
piration.
WOUNDS
To protect the wound from contamination
Objective
and control bleeding.
Definition
A wound is a break in the skin or mucous membrane.
It is caused by force and usually extends into the under-
lying tissue. Wounds may be classified into four types.
1. Abrasions, made by rubbing or scraping. Floor
burns or scuff burns, although called burns, are
true wounds.
2. Incised wounds, sharp cuts that tend to bleed freely.
3. Lacerated wounds, jagged or
irregular wounds,
often associated with much tissue damage.
4. Puncture wounds. A tack, run through the skin,
makes a typical, small puncture wound.
Wounds are subject to infection and bleeding. Deep
wounds may be complicated by injury to internal organs
and by fractures.
Prevention
Wounds are common accidental injuries, but many
can be prevented. Some measures might include:
Fig. 3 Four types of wounds
A. Abrasion B. Incised
C. Lacerated
D. Punctured
1. Keep firearms and ammunition under lock and key.
2. Keep knives, scissors, and other sharp implements
in a special storage place, well out of reach of small children.
3. Caution children about running while carrying
sharp instruments and about running against glass doors.
4. Put razor blades in a closed container where chil-
dren cannot find them.
5. Take special care when using knives or other sharp
WOUNDS
implements. Always hand a knife to another person
with the point turned away from the recipient.
6. Be especially careful in handling such equipment
as power mowers or power tools. Follow instruc- tons carefully.
7. Make sure that broken glass is swept up promptly. Infection
The growth of harmful germs in a wound constitutes
a wound infection. The germs destroy tissue about them.
Some kinds liberate poisons (toxins) that are carried
throughout the body, causing fever, and systemic injury.
Germs are everywhere about us in great numbers.
Some kinds are not harmful to man. Few can penetrate the
intact skin; but when a break, however tiny, occurs in the
skin, there is danger of infection. The body, like virtually
all objects about us, has a coating of germs. Therefore a
penetrating object carries in its own supply of germs and
also pushes some from the skin and perhaps the clothing into
the wound.
Evidence of infection does not appear at once after
injury, because the germs need some time to grow and
multiply. The evidence usually appears from two to seven
days or more later. The wound area becomes tender, red,
warm, and swollen; sometimes pus appears. Pus consists of
white blood cells, germs, and tissue debris. White blood cells,
like certain body chemicals, aid in fighting germs. Some-
times red streaks extend from the wound up the arm or leg,
and there may be tender nodules (small lumps) in the arm-
pit or groin. These indicate that certain drainage channels,
the lymph vessels, are also infected and show that the infection
is spreading. Fever and headache are often asso.
cited with infected wounds.
The tiniest wound permits entrance of thousands of
germs. Any wound, no matter how small, should have ade
quote attention. The man who boasts that he never has had
an infection has merely been fortunate. In the past, he hap.
pened to have resistance against the germs that entered his
wounds. Tomorrow he may meet a different variety. How.
ever, self-treatment is occasionally resorted to.
Wounds of the palms, of the lower extremities below
the knees, or the face, and those overlying joints involve
greater than usual danger. If infection develops in these
areas, results may be grave. Diabetics, and those with hardening
of the arteries or other circulatory disease, especially
should beware of infection in the lower extremities.
First Aid
Wounds in which bleeding is not severe
Home care for minor scratches. The best source of in-
formation concerning home care for minor scratches is
the family physician. Lacking such advice, the following
procedure may be followed if you elect to assume personal
responsibility and the risks of home care:
1. Wash your hands thoroughly with clean water and soap.
2. Cleanse the injury thoroughly, using plain soap
and boiled water cooled to room temperature or
clean running tap water and soap, applying the
soap and water with a sterile dressing. Sterile
dressings are described below.
S. Apply a dry sterile, or clean dressing, and bandage
it snugly into place.
4 Toll the patient to see his doctor promptly it evidence
of infection appears.
First aid preliminary to medical care. Usually the only
procedure should be to apply a sterile or clean dressing an
bandage it into place. Exceptions are noted with special
wounds later. The term "dressing," as used in this textbook
refers to the material that is placed directly over the wound,
and "bandage" means the material used to hold the dressing
in place. Sterile dressings are entirely free from germs. Such
dressings are available commercially in protective packets.
Care must be taken lest the dressing be contaminated with
germs while you apply it. The hands, the outside of the
packet, and any object touched by the dressing harbor
germs. Therefore wash your hands first. Upon opening the
packet, grasp the dressing by one corner and place it over
the wound so that the corner you touched does not overlie
the wound. Do not cough or breathe closely upon the
dressing. Dressings should be large enough to extend well
beyond the wound edges; remember that they may slip.
Then bandage the dressing into place. Bandages should
be clean, but not necessarily sterile. They should be snug,
but not tight enough to impede circulation.
If sterile dressings are not available, use a clean fabric,
with at least four layers over the wound. If possible, treat
the fabric to remove at least some of the germs. You can
scorch it with a flame, iron it, heat it under close observa-
tion in a hot oven, wash it with soap and water and then
ay it thoroughly, Or expose it for at least ten minutes to
re direct rays of the sun. The best method is to boil the
fabric for a few minutes, and then dry it. Fluff cotton
Should not be placed upon a wound; the fibers are hard to remove.
Wounds in which bleeding is severe
The objective is to stop the bleeding at once, always if
possible with pressure directly over the wound with a cloth.
You may save a life by controlling hemorrhage. If a
large blood vessel is cut, blood loss may be sufficient within
less than a minute to cause death; but in most cases, body
protective mechanisms soon cause some diminution
of bleeding. Sometimes, when a limb is severed by a crushing
force, there is surprisingly little bleeding, because the cut
ends are closed by the force and clots form. The ends may
reopen when the blood pressure rises again. The average-
size male has about six quarts of blood, the female somewhat
less in proportion to size. Adults can withstand readily the
loss of a pint, the amount usually taken for transfusion
purposes. Loss of over a quart of blood may be serious,
especially in the aged and debilitated.
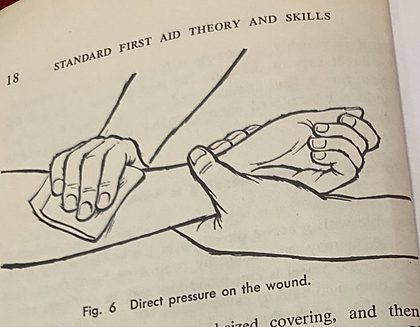
Direct pressure. Most external bleeding can be con-
trolled by applying pressure directly over the wound. Use
a clean cloth or a part of the clothing in real emergencies.
The cleaner and more nearly sterile the cloth the better
in preventing infection. Application of the bare hand may
be necessary for quick action in stemming a major blood
loss until effective cloth material can be brought to use.
Alter the bleeding has been controlled, apply additional
Fig. 6 Direct pressure on the wound.
layers of cloth to form a good-sized covering, and then
bandage snugly or firmly. Do not remove the dressing. If
blood saturates the dressing, apply more layers of cloth, and
perhaps tighten the bandage directly over the wound.
Pressure to the supplying vessel. For especially quick
action, in some cases you can use your fingers or the heel of
your hand to press the supplying vessel against the under-
lying bone. Such pressure causes the bleeding to diminish,
but does not stop it entirely. Meanwhile you or your assist-
ants can start measures to apply pressure directly over the
wound, as described above.
There are only two points on each side of the body
where pressure against the supplying vessel is of occasional
practical use: (1) Pressure on the inner half of the arm,
midway between the elbow and the armpit, compresses the
main vessel against the bone there and diminishes bleeding
in upper extremity below the point of pressure; (2) pres-
sure applied just below the groin on the front, inner half,
of the thigh compresses the main vessel against the under-
lying pelvic bone. If pressure is applied, bleeding should
diminish in the extremity below the point of pressure.
Summary: Bleeding can almost always be controlled
by direct pressure with a pad of cloth over the wound. In
case of severe wounds of an extremity, compression of the
main supplying vessel against the underlying bone may be
helpful for quick, temporary, partial control until cloth
for direct pressure is obtained. Use of a tourniquet in case
of hemorrhage from an extremity is justifiable only rarely.
If a tourniquet is applied for much over 2 hours, its release
may precipitate shock. This fact emphasizes the need for
promptness in getting a tourniquet patient to the hospital.
He deserves a high priority for transportation. The decision
to apply a tourniquet is in reality a decision to risk sacrifice
of a limb in order to save life.
The principal objective is to stop the bleeding at once.
This almost always can be done with a cloth pad held
directly over the wound. The first aid steps are these:
Stop the bleeding quickly.
Bandage firmly into place the cloths used in controlling
hemorrhage.
If an extremity is involved, elevate it, using pillows or
substitutes.
If there is delay in obtaining medical care and if the
patient is thirsty, give water as tolerated (approximately
½ glass every half hour)-provided there is no penetrating
wound of the abdomen or lower chest. Do not give alco-
holic drinks.
Internal bleeding
The signs are similar to those for shock, and the first
aid is the same. Shock is discussed in a separate chapter.
sometimes blood comes from the mouth and nose,
though no injury is noted in these organs. The bleeding point
probably is in the lungs, stomach, within the skull, or the
passages related to them. Provide pillows to raise the head
and shoulders if there is breathing difficulty. Try to have
the patient control vomiting movements. Give no stimulants
even though the bleeding ceases. Medical care
is urgently needed. If the patient is in shock or unconscious,
turn him on his side, with head and chest lower than hips,
to prevent aspiration into the lungs.
Nosebleed
Nosebleeds may occur spontaneously or as a result of
injury. There may be an underlying disease, such as high
blood pressure, but in many cases there is no disease. Some
people, particularly in youth, are often affected following
activity, colds, and exposure to high altitude. The bleeding
usually is more annoying than serious. Occasionally with
underlying disease the bleeding is profuse, prolonged, and
dangerous.
The person should remain quiet. A sitting position
with head thrown back, or a lying position with head and
shoulders raised is best. Walking about, talking, laughing,
or blowing the nose may cause increased bleeding or re-
sumption of bleeding.
Usually the bleeding area is near the tip of the nose.
Pinching the nostrils together puts pressure upon this area.
It may be necessary to pack the bleeding nostril lightly and
then pinch. It may be necessary to maintain pressure with
a small amount of gauze for several minutes, occasionally
the face, stop the bleeding.
Special wounds
The following general principles apply to all wounds:
prevent contamination, control hemorrhage, and provide
protection. Special wounds are considered at greater length
in the Advanced Course. However, selected points deserve
mention here.
Infected wounds. Infected wounds should have medi-
cal care. Do not pinch the wound and do not open the
wound with a "sterile" needle that has been passed through
a flame. First aid measures include:
1. Provide rest for the patient. Physical activity
favors the spread of infection.
2. Immobilize the affected part. Constant motion
of infected fingers, hands, feet, or neck, for example,
is harmful.
3. Elevation of an infected extremity, by placing
pillows beneath, may be of value. Infections of the
lower extremities subside more quickly if the patient
has complete bed rest than if he is up and about.
4. Sometimes it is impossible to obtain medical
help or advice for many hours. In such cases, wet appli-
cations may be administered. Use boiled water to
which 2 level teaspoonfuls of salt have been added per
quart of water. It is safest to use them at room temperature;
they may, however, be warm but never hot.
Immerse a towel in the solution and wring it out thoroughly
to guard against the frequent mishap of burn-
ing the patient. Then apply to the infected wound. A
dry towel may be placed outside the wet one. Observe
carefully lest a burn develop. Remember that although
the towel may not seem too hot when quickly handled,
it may cause a burn because of the long contact period.
The
applications may be
continued for half-hour
periods with alternate free periods of the same length.
Test the temperature of the water by your ability to
hold the full container in your hand without dis-
comfort from the heat.
Gunshot wounds
Always consider the possibilities of
fracture and internal organ injury. If the chest is penetrated,
bandage firmly or snugly over the skin injury to
prevent entrance and exit of air. B-B shot, embedded in the
skin, are extremely difficult to feel or detect. Advise the
doctor so that he may have X-rays taken if their presence
is suspected. Police must be notified.
Wounds with danger of tetanus. The danger of teta-
nus (lockjaw) should be considered in ALL WOUNDS.
Puncture wounds, especially those contaminated with barn-
yard soil or manure probably have the highest incidence of
tetanus but many cases of tetanus result from wounds so
insignificant that the patient does not recall them until
specifically questioned. The particular need is for medical
attention and possible immunization against tetanus. The
danger of tetanus illustrates one of the reasons why even
the most insignificant wound should be cleansed without
delay.
Animal bites. If a person is bitten by a stray animal,
call the police, doctor, and veterinarian immediately. The
animal should be restrained or prevented from escaping
until their arrival. The bites may cause the usual kinds of
infections. In addition, the bite of any warm-blooded ani
mal may cause rabies if the animal harbors the germs of this
discase. The disease appears to be invariably fatal in man,
once it develops. In this country, the dog, and less often, the
cat, skunk, fox, wolf, coyote, and other animals, may be
infected. Whenever suspicion of rabies danger exists, the
patient should have medical attention at once, and if necessary,
the immunization treatments to prevent the disease.
The dog should not be killed unless it is essential to protect
others from being bitten. The dog should be confined and
observed, preferably at the facilities of a veterinarian or
dog pound for the presence of rabies.
SHOCK
To prevent or reduce shock by keeping
Objective
the victim lying down and comfortable.
Definition
Shock is a term used with many meanings. Of most
importance to first aiders is traumatic shock, which is a
depressed condition of many of the body functions due to
failure of enough blood to circulate through the body fol-
lowing serious injury.
Decidedly different conditions are electric shock, dis-
cussed elsewhere in this textbook; insulin shock, caused by
an overdose of insulin; the temporary shock of simple
fainting; and the psychiatric condition formerly called shell
shock.
Causes and Dangers of Shock
Traumatic shock is associated with injury to body
tissue from burns, wounds, or fractures. In most instances
it is caused by loss of large quantities of blood either externally
or into the tissues of body parties, In General, uh.
beater the damage to flesh and bong, and the larzer"),
blood loss, the greater the danger that shock will occulif
"Shock may be produced of made worse by any manipulation
that increases hemorrhage or causes it to recut
Rough handling of the patient should be particular,
avoided. The aged and the debilitated do not withstand
shock as well as others.
If a person develops shock and remains in it, dealt
may result even though the injury causing the shock would
not be fatal otherwise. Therefore, proper first aid to help
prevent or to deal with shock is essential when caring for
any seriously injured person.
Signs and Symptoms of Shock
The most important evidence is the victim's weakness,
coupled with a skin that is pale and moist and cooler than
it should be.
Beads of perspiration may be noted about the lips,
forchead, palms, and armpits. The patient may vomit or
complain of nausea. His mental reactions may appear nor-
mal at first. Later, he may be restless or lose alertness and
interest in his surroundings. Thirst is commonly present.
The pulse is fast but may be weak or impossible to
feel. The patient may breathe faster than usual and occa-
sionally take deep breaths. These signs may not appear at
Especially in cases of severe hemorrhage, they may
develop only after an hour or more.
Shock should not be confused with simple fainting.
Individuals with minor injuries may faint. Even persons
who have not been injured may faint at the sight of a seri-
ous accident, particularly if blood is visible. One who has
fainted will be pale and often covered with perspiration.
He may be nauseated. The pulse will usually be slow. If he
is allowed to lie flat, recovery will occur promptly.
Since the evidence of shock may not be present, even
when the injuries are severe, the first aider may fail to apply
proper measures. The victim may seem alert and react
optimistically, but suddenly he may collapse. Sometimes
only a few signs of shock are noted, and the first aider may
think there is little need for concern. He may even permit
transportation of the victim in the sitting-up position. The
proper course is simple: give first aid for shock to all seriously
injured people.
First Aid for Shock
The same first aid measures apply to both prevention
and care of shock.
Position
Keep the patient lying down. The ling-down pogi
Lion favors the how of a greater amount of blood to the
bild and chest, where it is needed. Most. It places felt
demand upon the body than the sitting or standing post
lions: It is the most favorable position if there is injury to
internal organs and the head, or in case of a fracture. There
is one exception to the horizontal position: if there is dif.
culty in breathing, the patient's head and chest should be
elevated.
Except as noted below, elevate the lower part of the
body if the blood loss is great, or the injury severe. Raise
the foot of the bed or stretcher eight to twelve inches. If
the victim is on the floor or ground, place pillows or sub-
stitutes beneath the lower extremities. This elevation should
not be done: (1) if there is a head injury, (2) if breathing
difficulty is thereby increased, or (3) if the patient com-
plains of pain when it is attempted, such as pain at a frac-
ture site in the lower extremity or abdominal pain. For
lesser injuries, such as a fracture of the wrist, elevation is
unnecessary, though not harmful.
Heat
If the victim is lying on the ground or floor, place a
blanket beneath him. Cover him only sparingly, according
to the temperature of the environment. Do not cause
sweating. It is better if he is slightly cool than toasting
warm. On warm days little or no surface covering is needed.
Application of external heat by hot water bottles and
heating pads is usually harmful in shock. They may be used
in cold weather, if sufficient blankets are not available to
prevent freezing. If so, use utmost care not to burn the
patient. Remember that you test the warm object for only
a second or so, whereas it may be in contact with his skin
for a long time. Normally his skin will not withstand heat;
further, he usually does not recognize that a burn is de-
eloping, whether he is unconscious or not. The warm
object should have a temperature only slightly above body
temperature.
The overall principle relating to heat in shock is this:
do not add heat; simply prevent a large loss of body heat.
Flush the patient will be under medican, Within a hay
hour br less, the first alder need not concern himself wit
horas except to allay thirst. Fluids have, value in sheol
Auerheles; they should not be given, if the patient",
Nicornsious or only partly conscious, if he is nauseated
has a penetrating abdominal wound, or probably face
early operation.
"Plain water, neither hot nor cold, is the best Quid
Other drinks may cause nausea, a feeling of fullness, and
Dicoups. Do not give alcoholic drinks. A set rule concerning
the amount of fluid to give cannot be stated, because indi
vidual cases vary so much. If there will be delay until
medical care is available, administer a few sips at first.
Observing the patient's tolerance and thirst, increase the
amount to a half glass at a time. In case of large blood loss,
the patient is usually thirsty and will take drinks at short
intervals. Your concern should be to see that he does have
fluids, but at such doses and intervals that he does not vomit.
If he vomits or is nauseated do not give fluids. If medical
care will be unavailable or considerably delayed, give half-
glass doses of water, to which has been added one-half level
teaspoon table salt and one-half level teaspoon of baking
soda per quart, at about 15-minute intervals. Within an
hour medical advice should be obtained.
The problem of fluid administration is not great in
first aid usually, because the patient will have medical
attention fairly soon.
Other measures against shock
The underlying injuries should receive attention; for
example, hemorrhage should be controlled and fractures
splinted. The victim should not be disturbed by unnecessary
questioning, manipulation, and noise. Tactful encouragement
should be given. Stimulants such as ammonia or
coffee have no value in traumatic shock.